

My BRAIN STEM STROKE was very rare and caused serious permanent disabilities. The brain stem is in charge of all the functions your body needs to stay alive, automatic activities like breathing, digestion, and circulating blood. My type of brain stem stroke damaged nine of my twelve Cranial Nerves. Several of those nerves affected me being able to control most of the muscles in my body. This included muscles that are necessary for speech like the diaphragm, vocal cords, tongue, lips and just about all of the facial muscles. My limbs technically were not paralyzed but extremely close to it. It was strange because I still had sensation everywhere. It felt like I had weights all over my body holding me down. I was so weak that I was essentially quadriplegic. I was living everyone’s worse nightmare; I could not move nor could I speak! I was LOCKED-IN! Locked-in means that you aware of what is going on around you but you cannot move or speak due to lack of muscle control below the eyes.
I had my stroke while on business in Toulouse, France. The French doctors probably saved my life but they cared little about communicating with me. We had essentially NO COMMUNICATION. They only came in my room during rounds to look at me and read my chart. Sometimes they might write something for the nurses in my chart. Other than for them to do that I never saw them! They initially cared for me until my health stabilized. Once my health improved enough to travel I was put in a MedJet and flown back to the states.
After arriving back in an American hospital, one of the hospital staff’s goals was for me was to just have simple communication. Doctors and nurses spoke to me but they just asked me yes and no questions. My communication technique was limited to BLINKING my eyes once for yes or twice for no. I was scared to death that yes and no blinks is what my life was reduced to.
I was in two acute care hospitals during the first three weeks after my stroke until my condition stabilized. Next, I was transferred from an Acute Care to a Rehabilitation hospital. Acute care gives you medical attention while you are sick, which is right after your stroke. Rehabilitation hospitals have the task of helping you relearn to walk, talk and things like how to perform personal hygiene or how to dress yourself. Teaching me to communicate beyond eye blinks was one my rehab doctor’s biggest concerns. This was addressed almost immediately.
The first thing my Speech Language Pathologist (SLP) did was to make a COMMUNICATION BOARD for me. There are many types of Communication Boards. Some boards are made by the SLP and some can be purchased in a store. Mine was fabricated from 1/8” thick Plexiglas. It was approximately 18” wide by 24” long. My SLP stuck 2” letters of the alphabet on it. The person I was communicating with would stand about 2’ away and I would stare at a letter on the board. They would look at my eyes through the Plexiglas and track my gaze to that letter and call it out to me. I could say anything by staring at letters on a piece of Plexiglas board and spelling out sentences. My wife and I became extremely proficient at communicating by this means. She could anticipate my needs and what I was trying to spell. Communication was cumbersome but it soon became a common way for me to talk.
I actually had another form of communication while I was an in-patient at the rehabilitation hospital. It was very effective and I used it more often than my Communication Board. Most nurses did not know how the Communication Board worked. It definitely was not the nurses fault. All of my nurses were great. They gave me special care because I was quadriplegic. During the day shift I was out of my room doing therapy. By the time I returned to my room the shift had changed. Second shift nurses were usually scrambling like crazy to take care of other patients. And third shift nurses did not have anybody to show them how to use the board. So, I developed MY OWN METHOD to communicate. If I needed something in my room like the television turned on or off I would STARE at it. If my head hurt and I wanted Tylenol I would BLINK my eyes real fast several times. By staring or blinking I communicated quite effectively with the nursing staff.
About three months later, I was finally discharged from the rehab hospital and sent home. I took the Communication Board home with me. For months, it was still my primary form of communication.
One day, while sitting at home watching TV I suddenly had the urge to push my legs. At first, I just thought I had muscle spasms in my legs. But then, I felt that I could make my leg muscles fired on command. It is not uncommon for muscles to suddenly wake up months after a stroke. I discovered that this new muscle control allowed me to push and extend my legs. If I was in bed, lying in the fetal position, I could push my legs straight. If in my wheelchair, I could push and try to straighten my legs, which would force my feet down into the wheelchair’s footrests.
I soon discovered that if I just PUSHED MY FEET INTO THE FOOTRESTS I was able to push a faint sound out of my mouth! This was really exciting! For nearly a year I could not conjure up a peep. Now, I accidentally figured out how to make a sound on demand. I demonstrated this technique to my out-patient SLP and she became thoroughly intrigued. She theorized that pushing my leg muscles into the footrests was causing my whole body to tense up. This gave me the strength to take a breath and force air from my diaphragm. In turn, when I tightened my throat it caused my vocal cords to close enough to slightly vibrate. This created a faint but distinct sound from my mouth.
The key to remember is that I was not technically paralyzed. This fact is what made the progression with my speech even possible. My muscles were extremely weak but I could still control their movement with my mind. Pushing my feet against my footrests gave my other muscles just enough strength that I could coordinate making my diaphragm take a small breath in and forcing a small breath out. I had to coordinate bearing down on my legs, pushing out as much breath as I could and at its peak think about tightening my throat, as I exhaled, so my vocal cords could move together. Also, making a sound did not happen spontaneously like it does in able-bodied people. Each of my muscle movements required an individual thought. I had to effectively learn everything from the beginning. It required patience, extreme concentration and lots and lots of practice!
My SLP formulated a plan for getting me to talk again. Whenever I wanted to try talking I would push my legs. I practiced this method every day and soon learned how to pronounce several words. Pronouncing words is much more complex than just making a sound. I had to go through all the coordination of motions that I explained was necessary to make a sound but now I had to think about making my facial muscles move so I could purse my lips in umpteen different formations while trying to put my tongue in the proper configuration.
Certain words were impossible to pronounce no matter how hard I tried. I could not make my tongue lift up or stick it out very far. Words with the single consonant letters c, s or t and words with the consonant blends, such as bl, ch or spl were out of the question.
One day, my wife was browsing through a magazine about physical therapy. She happened to read an article written by a physical therapist that had a brain stem stroke similar to mine. The therapist had also lost her speech. She was slowly regaining it but was also struggling pronouncing words with certain sounds and blends. Her SLP recommended that she use something called a PALATAL LIFT PROSTHESIS to help her speak. The Palatal Lift is an oral prosthetic like a denture. The way she explained it was that her stroke caused her soft palate to fall from its normal position.
My wife and I were very excited about the Palatal Lift. It sounded like its purpose was for people that had problems with their soft palate, like me. We spoke to my SLP but she did not know much about them. In the meantime, I kept practicing saying the words I could pronounce using my pushing technique. This went on for a couple of months but there were still those sounds I could not make.
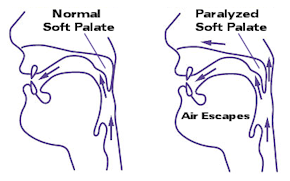 One day, at my Speech Therapy session, my SLP wanted to check to see if air was escaping out of my nose while I was trying to talk. She brought out what looked like a GIANT PLASTIC CLOTHES PIN with pads that covered the area that went over the nostrils. It closed gently but with enough force to pinch off the nostrils although not hard enough to be uncomfortable. Immediately my speech improved! Most of those hard to pronounce words with certain consonants and consonant blends now came out clearly. I learned that if someone held my nose I could make those sounds. Apparently air was escaping out of my nose preventing me from making the sound I wanted. With this discovery, my Speech Therapist felt that maybe the Palatal Lift might indeed help. There was no guarantee but I was willing to try. Life without talking was too inconceivable. Besides, I looked pretty silly with someone holding my nose every time I wanted to talk.
One day, at my Speech Therapy session, my SLP wanted to check to see if air was escaping out of my nose while I was trying to talk. She brought out what looked like a GIANT PLASTIC CLOTHES PIN with pads that covered the area that went over the nostrils. It closed gently but with enough force to pinch off the nostrils although not hard enough to be uncomfortable. Immediately my speech improved! Most of those hard to pronounce words with certain consonants and consonant blends now came out clearly. I learned that if someone held my nose I could make those sounds. Apparently air was escaping out of my nose preventing me from making the sound I wanted. With this discovery, my Speech Therapist felt that maybe the Palatal Lift might indeed help. There was no guarantee but I was willing to try. Life without talking was too inconceivable. Besides, I looked pretty silly with someone holding my nose every time I wanted to talk.
We found a dentist who had experience making Palatal Lifts (actually he was a Prosthodontist). He made the form, which is like a plastic retainer, and with a few modifications I was able to start talking. I now could say almost anything. One physical problem still existed with me. My stroke caused something called Dysarthria. All the things which are required for normal speech are extremely weak. Breath support, lip strength, tongue lift, protrusion, facial muscles, all the things that you take for granted when you speak were severely affected. I can talk but it is very soft. I’ll take that though.
With the Palatal Lift, I was able to vastly expand my word list. I practiced every day. My breath support was still very weak, though. As hard as I tried, I could only say one word at a time. Every word I spoke my wife would pronounce the word back to me after I said it. This was necessary so I could confirm she understood what I was saying. If she said the wrong word, then I would shake my head no and I would say my word again. If I could not pronounce a word correctly and my wife could not figure out what I was trying to say she would ask me to I spell the word instead of pronouncing it incorrectly over and over. Pronouncing letters was much easier and clearer. I did not mind if it meant that I was being understood.
I seemed to still be recovering from my stroke. My wife, me and all of my out-patient therapists felt that another in-patient hospital stay might provide a more intensive therapy environment. My insurance company approved me for another in-patient therapy stay during the summer of 1996. My new SLP suggested that I receive an evaluation by an Ear, Nose and Throat (ENT) doctor. I went to my ENT and he evaluated my vocal cords with a video stroboscope. A video stroboscope was used to make a video of my vocal cord movement. The video gave my ENT the advantage of watching closely how well my vocal cords moved, plus he could show the video to others, too. The video showed that my vocal cords were not actually paralyzed. It showed that my cords tried to close but would stop short of coming together.
That accounted for the lack of vocal cord vibration and a whisper like voice. The ENT studied the video further. After reviewing the video with his associate they concluded that I was a candidate for bilateral implants, VOCAL CORD MEDIALIZATION. He explained that this operation is more frequently performed when one vocal cord is paralyzed but he had seen it done on both. He explained what the procedure was in detail.
PROCEDURE: First, he would make a horizontal incision from left to right across my neck. Then, he would fold back my neck skin so that he could perform the procedure on my vocal cords. Next, he would slice off small pockets, approximately ¼” long by 1/16” deep, from the cartilage on my cords. Then, he would fit small silicone implants into each pocket where he just cut the cartridge away. This would push the gap between the cords close enough together that they would vibrate when I talked but not too close that they would inhibit breathing. I would be given “twilight” anesthetic so he could ask me to speak during the procedure to make sure the implants were of the optimum thickness. Finally, he would close my neck skin over and stitch me up. He asked me if I wanted to try the operation. I whispered, yes.
I had my procedure at the end of 1996. The sound of my voice improved but was still very soft. Poor breath support prevented me from projecting my voice. I am sure that this procedure would work fine for anybody who could control their diaphragm. It helped me get a voice easier but the procedure was limited. I needed to be able to control my diaphragm if I wanted to speak normally again. What was neat was that I COULD TALK with a voice. I mean I could talk with a voice before but I had to push really hard with my legs. I still had to tense up each time I spoke and push initially, “kick starting” my voice, but after that the word came out easily.
Several years after my operation, something terrible and unexpected happened! It would change my life forever! It seemed like this happened out of the blue. I was in the fourth year after my stroke. My legs tingled after my stroke. I had just assumed that it was a side-effect of my stroke. How wrong I was! The tingling was slowly becoming extremely painful. My legs felt like I had bad sunburn. I suffered with this pain for several years. The pain was becoming progressively worse. I went to doctor after doctor. Nobody was familiar with the symptoms.
One day, my wife was reading a magazine about stroke. The person who wrote the article had symptoms similar as me. They were being treated successfully by a Pain Management Clinic. This type of pain had a name. It was called CENTRAL PAIN.
Unfortunately, Central Pain would ruin my life forever!
To be continued . . .
FOOTNOTE: Shortly after my stroke, I found that with the proper setup I could use my COMPUTER. I downloaded an ON-SCREEN KEYBOARD and purchased an INFRARED HEAD POINTER. This setup allowed me to type and move the cursor almost as well as most able-bodied people. I sent literally thousands of emails, hosted an America Online chat room for stroke support, taught myself HTML and created over a dozen websites, plus accomplished many more things. Since 1995, using the computer has been my most extensive form of communication! To learn about my various types of communication on the computer, read my blog article, Disability. . . Not on the Computer.
One more thing, when I say that I cannot talk I am sort of lying. The communication techniques I mentioned above caused me to practice forming words and attempting to pronounce them with voice on a daily basis. It also caused my wife and kids to try and figure out what I was saying to them. They had to watch my mouth several times daily, especially my wife, because she is my caregiver and is with me the most. They all practiced READING LIPS as often as I practiced MOUTHING WORDS. Eventually, it became easier for us if I just mouthed the words and not put the effort into saying them with voice. By this time, they were just reading my lips, anyway. After years and years of practicing how to form words with my mouth, I now just mouth words and my wife and kids read my lips. So today, I “talk” to my wife and kids regularly!
Filed under: Personal | 2 Comments »
